

Welcome to Amanda's NICU Education


Hi! My name is Amanda. I'm a NICU nurse, Clinical Nurse Specialist, NICU Educator... basically your NICU BFF. If you want to talk NICU, I'm here for you! I love everything about NICU nursing and I'm eager to learn and share my knowledge with all my NICU friends.
I have been a NICU nurse since 2009 I am currently a Clinical Nurse Specialist in a Level IV NICU in Los Angeles.
I am passionate about educating the next generation of NICU nurses. I share my knowledge through platforms such as Instagram and Facebook and am excited to have you here on my website!
Click on the button below to sign up for my newsletter filled with NICU education and tips for all experience levels.

Not very many people love taking tests but as a self-acclaimed "forever student" who has taken (and passed) five different certification exams I am no longer afraid of tests! "Way to brag", you might be thinking but I want to help YOU pass your certification exam too!
Introducing Amanda's RNC-NIC Success digital course - your ultimate study companion!
Gain unlimited, on-demand access for life, ensuring you're primed to ace your certification exam.
I'm here to help you succeed and I can't wait for you to share with me that you PASSED the RNC-NIC EXAM!!!








Steroids for BPD
"Can you explain the difference between dexamethasone and hydrocortisone for extubation?"
I received a great question the other day asking about the difference between steroids to facilitate extubation in the NICU. Hydrocortisone and Dexamethasone are both corticosteroids that can help facilitate extubation, but how do they work, what are the risks, and how does the medical team determine which steroid to give? Let’s review the evidence together.
Bronchopulmonary dysplasia (BPD) remains the most common morbidity of prematurity, affecting thousands of infants annually in the United States. BPD is a developmental disruption in lung growth and maturation. It manifests with decreased oxygenation, as well as increased work of breathing and susceptibility to pathogens and environmental factors. Two of the major factors that contribute to BPD are inflammation and mechanical ventilation, thus corticosteroids may be prescribed in an attempt to facilitate extubation and reduce pulmonary inflammation.
Pathophysiology
Before we dive into steroids, let's make sure we're all on the same page about BPD. If you've been in the NICU for a while, you've definitely seen it, but do you feel like you understand what's happening inside the lungs?
BPD occurs due to multiple factors including interrupted lung development, inflammation and lung injury due to mechanical ventilation.
The "Multi-Hit" Theory
Here's what I want you to remember for your RNC-NIC exam: BPD isn't caused by just one thing. It's what we call a "multi-hit" process:
Hit #1: Baby is born early because of infection, preeclampsia, or other complications
Hit #2: Immature lungs undergo injury due to mechanical ventilation
Hit #3: Oxygen exposure creates free radical damage
Hit #4: Maybe the baby gets an infection or develops NEC ☹️(which causes MORE inflammation)
Hit #5: More ventilator time, more inflammation...
Each "hit" makes BPD more likely, and unfortunately, many of our tiniest babies experience multiple hits.
RNC-NIC Tip: Remember that BPD is defined as needing supplemental oxygen at 28 days of life OR at 36 weeks postmenstrual age, depending on which definition your unit uses.

Yu et al, 2024
Why Do We Use Steroids for BPD?
Great question! Here's the thing—inflammation is a HUGE part of what drives BPD development. When we can reduce that inflammation in the lungs, we often see:
✅ Easier time weaning from the ventilator
✅ Less oxygen requirement
✅ Better lung compliance
✅ Reduced risk of severe BPD
Think of steroids as powerful anti-inflammatory medications that can help break the cycle of lung injury and inflammation.
Sounds great, right? So why is there hesitancy? Steroids have been known to reduce inflammation since the 1980s BUT further research found that the babies who received prolonged high doses of dexamethasone (especially early in life) had worse developmental outcomes (cerebral palsy, neurosensory disability, and poor growth). In the early 2000s, the AAP had a policy statement stating we should not routinely prescribe postnatal steroids.
A lot has changed since then. Smaller and smaller babies are surviving and BPD is still a major issue. More studies have been completed and the AAP has revised their statement (in 2010 then again in 2022) stating that postnatal corticosteroids cannot be routinely recommended and the decision to use corticosteroids to prevent or treat BPD must be individualized.
Individualizing Treatment: Who Should Get Steroids?
This is probably one of the most important and difficult questions. The research gives us some guidance, but every baby (and NICU) is different.
The Risk vs the Benefit
The baseline risk of BPD in your patient population matters.
Low baseline BPD risk (<33%): Using steroids actually increases the risk of death or cerebral palsy.
High baseline BPD risk (>60%): Steroids reduce the combined outcome of death or cerebral palsy.
So what does this mean for your NICU? Your team needs to identify babies who are at high risk for developing moderate-to-severe BPD. How do we do that?
Using the Neonatal BPD Outcome Estimator
Clinical Pearl: There's a fantastic tool called the Neonatal BPD Outcome Estimator that can help you calculate a baby's risk of BPD at various time points.
The Clinical Decision-Making Process
The evidence-based threshold of 60% moderate-to-severe BPD risk isn't always straightforward to apply because BPD risk actually decreases as babies get sicker (due to increased mortality risk).
What this means in practice: Centers need to individualize their treatment thresholds based on:
Local risk profiles
Family priorities and values
The specific clinical scenario
Neonatal BPD Outcome Estimator
Steroids for Prevention of BPD: What Does the Research Say?
Hydrocortisone:
What is it: Hydrocortisone is a corticosteroid that has both glucocorticoid AND mineralocorticoid activity. It is a steroid more similar to endogenous cortisol which makes it potentially safer than dexamethasone.
The PREMILOC Protocol (for early use): Consider if your unit's BPD rate is high (≥50th or 75th percentile)
Especially for infants <1000g exposed to chorioamnionitis
Started within 24 hours of birth
1 mg/kg/day divided twice daily for 7 days
0.5 mg/kg/day once daily for 3 days
Important: Cannot use with NSAIDs due to risk of perforation
Results: The rate of survival without bronchopulmonary dysplasia at 36 weeks of postmenstrual age was significantly increased by prophylactic low-dose hydrocortisone.
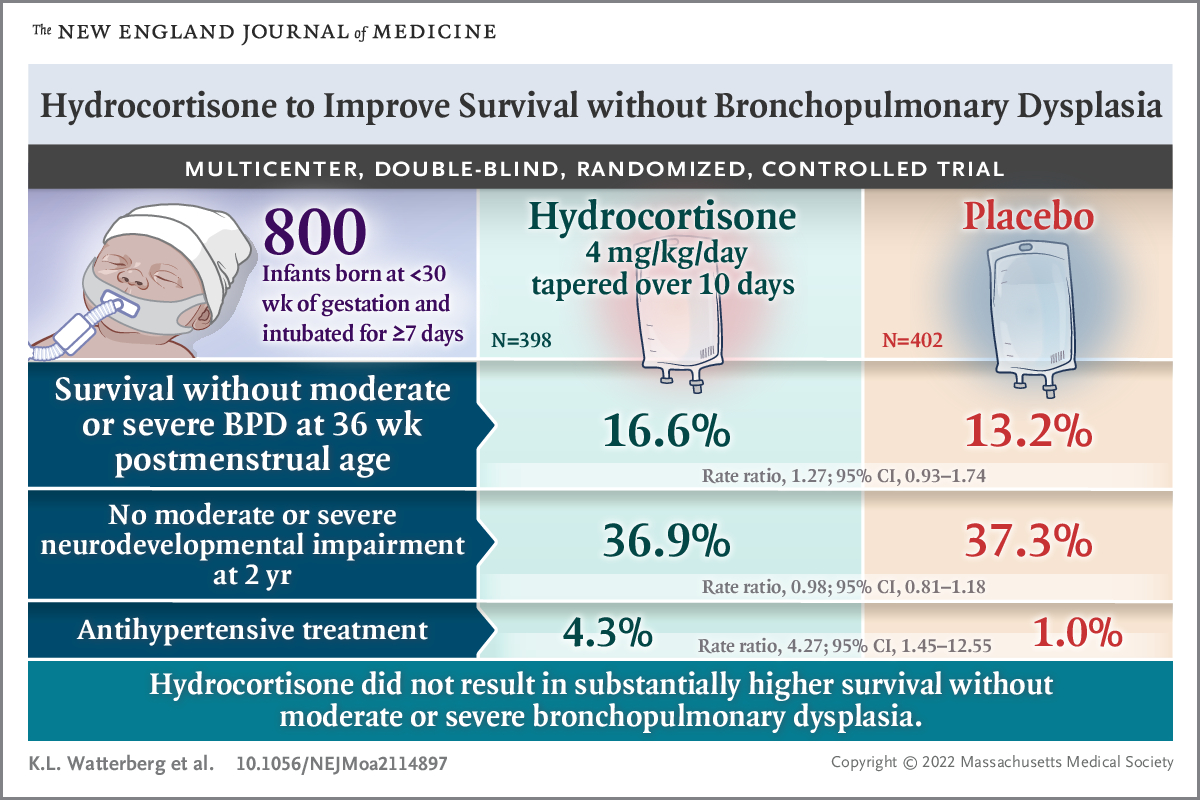
The STOP-BPD Protocol (for later use):
Started between 7-14 days of life, continuing for 22 days
Much higher doses than PREMILOC
5 mg/kg/day for 7 days, then taper
Results: Administration of hydrocortisone between 7 and 14 days after birth, compared with placebo, did not improve the composite outcome of death or BPD at 36 weeks’ postmenstrual age. However, there was a significant reduction in mortality by 36 weeks in the Hydrocortisone group.
Dexamethasone:
What it is: This is your most potent anti-inflammatory steroid, about 25 times stronger than hydrocortisone. Dexamethasone: A Randomized Controlled Trial (DART) examined using a short course (10 days) of low dose dexamethasone in infants at high risk (<28 weeks or <1000g who remained on mechanical ventilation after 7 days of life).
The DART Protocol:
Total dose: 0.89 mg/kg over 10 days
Day 1-3: 0.15 mg/kg/day divided twice daily
Day 4-6: 0.10 mg/kg/day divided twice daily
Day 7-8: 0.05 mg/kg/day divided twice daily
Day 9-10: 0.02 mg/kg/day divided twice daily
Results: This RCT showed low-dose dexamethasone treatment after the first 1 week of life facilitates extubation and shortens the duration of intubation among ventilator-dependent, very preterm/extremely low birth weight infants, without any obvious short-term complications. Of note, 85% of infants exposed to dexamethasone had BPD at 36 weeks (compared to 91% of placebo group). A modest reduction that is not statistically significant, though it is important to note the trial was stopped early due to low recruitment.
Key point: In practice, this protocol is typically started after 21 days of life when babies can't wean from the ventilator.
Prednisolone: For Established BPD
Prednisolone is typically reserved for babies who already have established BPD (after 36 weeks PMA) and are still requiring significant respiratory support.
Bhandari Protocol (shorter course):
2 mg/kg/day divided twice daily for 5 days
1 mg/kg/day once daily for 3 days
1 mg/kg/day every other day for 3 doses
Results: This observational study showed that oral prednisolone therapy is effective in weaning off supplemental oxygen in a postterm infant with oxygen-dependent bronchopulmonary dysplasia who has a pulmonary acuity score of < 0.5 and PCO2 of < 48.5 mmHg. In addition, if a single course of prednisolone fails, there is no clear benefit of using multiple courses.
Timing Is Everything: Early vs. Late Steroid Use
Early Use (< 7 days): BPD Prophylaxis
Here's what the research tells us:
Hydrocortisone: The PREMILOC protocol showed early low dose hydrocortisone showed a reduction in death and BPD, with no significant difference in the rate of cerebral palsy or neurodevelopmental impairment. Interestingly, the infants treated with hydrocortisone had significantly lower incidence of major cognitive impairment.
Dexamethasone: Should not be given in the first 7 days of life. The risks outweigh the benefits.
Late Use (> 7 days): Early Evolving BPD
Hydrocortisone: Might be preferred if given between 7 and 21 days of life since hydrocortisone may be safer for the brain.
Dexamethasone: DART protocol showed no increased risk for cerebral palsy or major disability (though there was a small sample size)
There is a gap in the research to compare hydrocortisone to dexamethasone at this point.
Clinical Tip: Many units use 21 days as their decision point. Before 21 days? Consider hydrocortisone. After 21 days? Dexamethasone becomes a reasonable option.
Nursing Assessment and Monitoring
What should you be monitoring for in your patient receiving steroids?
Glucose Issues:
Check blood sugars based on your NICU protocol
Be ready for insulin if glucose >180-200 mg/dL
Dexamethasone is notorious for causing hyperglycemia
Blood Pressure:
Monitor frequently (e.g. every 4-6 hours)
Steroids make the heart more sensitive to natural stress hormones
GI Complications:
Watch for feeding intolerance, increased emesis
Early hydrocortisone + indomethacin = HIGH risk for bowel perforation
Steroids and NSAIDs cannot be given together
Any signs of abdominal distension or bloody stools? Notify the medical team immediately.
Growth and Nutrition:
Close monitoring of growth and length is crucial
Does your unit use a length board?
Growth deceleration during treatment may occur
Recall that steroids may stunt growth
Work with your dietitians to maximize nutrition
Infection Vigilance
Remember: steroids suppress the immune system.
Infants exposed to postnatal corticosteroids have an increased risk of late onset sepsis (I would know this for the RNC-NIC or CCRN-N exam)
Be extra vigilant with hand hygiene and sterile technique
Watch for subtle signs of infection (they may not mount a typical response)
Temperature instability might be your first clue
Adrenal Suppression
When babies receive steroids for more than 14 days, their bodies can "forget" how to make their own stress hormones, like cortisol.
What Is Adrenal Suppression?
Infants are at risk for secondary adrenal insufficiency if they have been given supraphysiologic glucocorticoid doses for more than 14 days. Exogenous supraphysiologic glucocorticoids cause secondary adrenal insufficiency through effects on the hypothalamic-pituitary-adrenal (HPA) axis, the physiologic regulator of endogenous glucocorticoid production.
Signs to Watch For:
Hypoglycemia
Low blood pressure that doesn't respond well to fluids
Hyponatremia
Lethargy, poor feeding
Fluid retention
The Weaning Process
For babies on steroids ≥14 days, we can't just stop the steroids. Instead the steroids must be gradually tapered. Steroid tapers should be individualized to each patient and may range from a few days to several weeks or months, depending on the duration of steroid therapy
ACTH Stimulation Testing
What is an ACTH Stim Test?
Normally, adrenocorticotropic hormone (ACTH) is released from the anterior pituitary gland and travels to the adrenal cortex which causes the release of cortisol.
In an ACTH Stim test, a cortisol level is drawn shortly after administration of exogenous ACTH.
This allows us to assess the infants response to pituitary hormones.
When do we do this?
Babies who've been on steroids >14 days to assess adrenal response to ACTH.
Before stopping maintenance hydrocortisone
If we're worried about adrenal insufficiency
How it works:
Give 1 mcg of synthetic ACTH (cosyntropin) IV
Check cortisol levels at 0, 30, and 60 minutes (it is very important these are drawn at the exact time)
Normal response: Peak cortisol >18 mcg/dL means the adrenal glands are functioning normally.
RNC-NIC Pearl: Don't rely on random morning cortisol levels in babies—they don't have established circadian rhythms yet.
Family Education: What Parents Need to Know
Help families understand that:
BPD is a common complication of prematurity affecting lung development
Corticosteroids are powerful anti-inflammatory medications that may help reduce lung inflammation
The decision to use steroids involves careful weighing of benefits against potential risks
The goal is to help their baby wean from the ventilator and reduce long-term breathing problems
Setting Realistic Expectations
Discuss with families:
Timeline: Effects may not be immediate; improvement typically occurs over days to weeks
Monitoring: Their baby will need close monitoring for side effects
Uncertainty: Not all babies respond to steroid therapy
Long-term outlook: Some babies may still require oxygen or breathing support despite treatment
If Baby Goes Home on Steroids
Some babies might go home on maintenance hydrocortisone. It's important that families know how to give the maintenance medication and how important it is that babies do not miss a dose. In addition, it is important they understand:
Stress Dosing:
When baby is sick with fever, vomiting, or needs surgery, they need EXTRA steroid because their adrenal glands aren’t able to produce it on its own.
Hydrocortisone tablets can be crushed and mixed with a small amount of formula
Parents should be instructed on how to give IM injections in case the infant is unable to take the oral dose.
Red Flags: Teach families to call immediately for:
Persistent vomiting (can't keep oral meds down)
Severe lethargy
Any fever >101°F
Before any surgical procedures
As NICU nurses, we're often the first to notice subtle changes that might indicate steroid side effects OR signs that a baby is ready to wean respiratory support. Here are some things I want you to think about:
Questions to ask yourself:
How comfortable am I explaining to families why we're starting steroids?
Do I know the signs of adrenal insufficiency?
When should I be concerned about blood sugar levels in babies on steroids?
What does my unit's protocol look like for steroid weaning?
For your RNC-NIC preparation:
Know the different steroids that may be used to prevent BPD. What are the risks and benefits of each?
Understand the concept of adrenal suppression and how we monitor for it
Be familiar with side effects and nursing interventions
Remember that timing of steroid administration affects both efficacy and safety

In Summary
Steroids can be incredibly helpful tools in managing BPD, but they're not magic bullets. Every decision to start steroids involves weighing potential benefits against real risks. As the nurse caring for these babies, you play a crucial role in:
✅ Monitoring for both therapeutic effects and side effects
✅ Educating families about what to expect
✅ Recognizing early signs of complications
✅ Advocating for appropriate weaning and follow-up plans
Remember: you're not just giving medications, you're helping to optimize outcomes for some of our most vulnerable patients while keeping them safe throughout the process.
Want to dive deeper into BPD management? This is exactly the kind of complex topic we cover extensively in my RNC-NIC course. Understanding the nuances of steroid therapy, being able to explain the rationale to families, and knowing how to monitor for complications, these are the skills that set certified NICU nurses apart.
What questions do you have about steroid management in your NICU? I'd love to hear from you!
If you enjoyed this newsletter, I hope you'll share it with a friend! Let's learn together 🤓
Until next time,
Amanda 💛
Your NICU CNS + Study Buddy
Missed my other newsletters? Click here to read them!
References:
Cummings JJ, Pramanik AK; COMMITTEE ON FETUS AND NEWBORN. Postnatal Corticosteroids to Prevent or Treat Chronic Lung Disease Following Preterm Birth. Pediatrics. 2022;149(6):e2022057530. doi:10.1542/peds.2022-057530
Watterberg KL, Walsh MC, Li L, et al. Hydrocortisone to Improve Survival without Bronchopulmonary Dysplasia. N Engl J Med. 2022;386(12):1121-1131. doi:10.1056/NEJMoa2114897
Baud O, Maury L, Lebail F, et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): a double-blind, placebo-controlled, multicentre, randomised trial. Lancet. 2016;387(10030):1827-1836. doi:10.1016/S0140-6736(16)00202-6
Onland W, Cools F, Kroon A, et al. Effect of Hydrocortisone Therapy Initiated 7 to 14 Days After Birth on Mortality or Bronchopulmonary Dysplasia Among Very Preterm Infants Receiving Mechanical Ventilation: A Randomized Clinical Trial. JAMA. 2019;321(4):354-363. doi:10.1001/jama.2018.21443
Doyle LW, Davis PG, Morley CJ, McPhee A, Carlin JB; DART Study Investigators. Low-dose dexamethasone facilitates extubation among chronically ventilator-dependent infants: a multicenter, international, randomized, controlled trial. Pediatrics. 2006;117(1):75-83. doi:10.1542/peds.2004-2843
Bhandari A, Schramm CM, Kimble C, Pappagallo M, Hussain N. Effect of a short course of prednisolone in infants with oxygen-dependent bronchopulmonary dysplasia. Pediatrics. 2008;121(2):e344-e349. doi:10.1542/peds.2006-3668
McNerney KP, Arbeláez AM. Steroid Use in the NICU: Treatment and Tapering. Neoreviews. 2023;24(4):e207-e216. doi:10.1542/neo.24-4-e207
Liguori, M., Croop, S., & Trembath, A. Bronchopulmonary Dysplasia. Fetal and Neonatal Pharmacology for the Advanced Practice Nurse. Springer Publishing Company; 2023.
Rostas SE, McPherson C. Systemic Corticosteroids for the Prevention of Bronchopulmonary Dysplasia: Picking the Right Drug for the Right Baby. Neonatal Netw. 2016;35(4):234-239. doi:10.1891/0730-0832.35.4.234
Doyle LW, Cheong JL, Ehrenkranz RA, Halliday HL. Early (< 8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst Rev. 2017;10(10):CD001146. Published 2017 Oct 24. doi:10.1002/14651858.CD001146.pub5
Yu H, Li D, Zhao X, Fu J. Fetal origin of bronchopulmonary dysplasia: contribution of intrauterine inflammation. Mol Med. 2024;30(1):135. Published 2024 Sep 3. doi:10.1186/s10020-024-00909-5
Greenberg RG, McDonald SA, Laughon MM, et al. Online clinical tool to estimate risk of bronchopulmonary dysplasia in extremely preterm infants. Arch Dis Child Fetal Neonatal Ed. Published online June 21, 2022. doi:10.1136/archdischild-2021-323573

Copyright © {{right_now.year}} {{location.name}}, All rights reserved.


December 2023 Certification Review Webinar
NICU Certification Review


Ready to kickstart your journey to becoming a certified NICU nurse?
Look no further!
Grab my FREE E-Book packed with essential study and test-taking strategies for the RNC-NIC.
In the E-Book I give you the resources you need including the link to access the candidate guide, several types of books to study from, some of my favorite strategies, an outline of the content you should review, and a blank calendar for you to make your study plan!
Frequently Asked Questions About the RNC-NIC exam

What is the RNC-NIC?
The RNC-NIC is a competency-based exam that tests the specialty knowledge of nurses in the United States & Canada who care for critically ill newborns and their families.
The RNC-NICU is a nationally recognized certification that recognizes the registered nurse for their specialty knowledge and skill.

Who can take the RNC-NIC exam?
Nurses can take this exam after a minimum of two years experience in the NICU caring for critically ill newborns and their families.

Which books should I use?
I'm glad you asked! There are many excellent books to help you prepare for the RNC-NIC, I gathered ande describe each of them for you in my FREE e-book.
Is there a course to help me study?
Yes! Many hospitals host their own certification course and there are a few online courses. See my RNC-NIC test taking tips E Book for more information
What happens if I don't pass the exam?
If you don't pass the exam on your first try you can try again after 90 days. You will have to reapply after 90 days and pay a retest fee. There is no limit to the number of times you can take the exam (however a candidate can only sit for the exam twice per year).

Can I make more money if I take the RNC-NIC exam and get certified?
Yes! Many hospitals provide a raise or a bonus for nurses with specialty certifications. Hospitals also typically hire at a higher base salary when nurses have a certification.

Find me @amandasnicued on these channels or Email me
hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]