

Welcome to Amanda's NICU Education


Hi! My name is Amanda. I'm a NICU nurse, Clinical Nurse Specialist, NICU Educator... basically your NICU BFF. If you want to talk NICU, I'm here for you! I love everything about NICU nursing and I'm eager to learn and share my knowledge with all my NICU friends.
I have been a NICU nurse since 2009 I am currently a Clinical Nurse Specialist in a Level IV NICU in Los Angeles.
I am passionate about educating the next generation of NICU nurses. I share my knowledge through platforms such as Instagram and Facebook and am excited to have you here on my website!
Click on the button below to sign up for my newsletter filled with NICU education and tips for all experience levels.

Not very many people love taking tests but as a self-acclaimed "forever student" who has taken (and passed) five different certification exams I am no longer afraid of tests! "Way to brag", you might be thinking but I want to help YOU pass your certification exam too!
Introducing Amanda's RNC-NIC Success digital course - your ultimate study companion!
Gain unlimited, on-demand access for life, ensuring you're primed to ace your certification exam.
I'm here to help you succeed and I can't wait for you to share with me that you PASSED the RNC-NIC EXAM!!!








Neonatal Shock
What's happening during Shock, and what do NICU Nurses need to know?
September is always a special month for me, did you know its NICU Awareness Month? Every year, this month gives me a moment to pause and reflect on why I’m so grateful to be part of this extraordinary community.
I still remember the very first time I walked into a NICU as a nursing student. I had no idea this world even existed. But watching the resilience of those tiny babies, the strength of their families, and the dedication of the nurses around me lit a fire in me that has never gone out. From that day forward, I knew this was my calling.
Since then, I’ve been shaped by the NICU in ways I never could have imagined. It’s taught me patience, kindness, and the importance of the little things—because in the NICU, something as small bringing the hands to the face can have lifelong impact. It’s shown me what true love and perseverance look like, through families who show up day after day, giving everything for their babies.
Most of all, I’m grateful for the community—the NICU nurses who came before me and taught me, the colleagues who inspire me daily, and the families who trust us with their most precious little ones. If I had to sum it up, the NICU is about love, strength, and community.
💜 This NICU Awareness Month, I want to say thank you. Thank you for everything you do, for every baby step you take alongside families, and for being part of this mission to provide the very best care.
👉 Share this newsletter with a NICU nurse who inspires you, and let’s celebrate the incredible NICU community together.
Invest in yourself with the Certification Review Course
Neonatal shock remains one of the most challenging conditions we encounter in the NICU. While we often focus on blood pressure as our primary indicator, the underlying physiology is far more complex than a single number can capture.
Neonatal Shock
Shock occurs when oxygen delivery fails to meet tissue demand. In neonates, this presents unique challenges due to developmental differences in cardiovascular physiology. Unlike adults, preterm infants have immature myocardium with limited contractile reserve and underdeveloped autoregulation mechanisms.
The traditional approach of equating hypotension with shock oversimplifies the problem. As recent research demonstrates, many hypotensive neonates maintain adequate organ perfusion through compensatory mechanisms, while others with "normal" blood pressure may have compromised tissue oxygenation.

🔬 Normal Physiology: Oxygen Delivery & Uptake
Under normal conditions, the cardiovascular system’s main job is to deliver oxygen to tissues. Remember, cardiac output (CO) occurs thanks to heart rate (HR) and stroke volume (SV).
CO = HR x SV
The SV is the volume of blood ejected from the left ventricle (LV) and it is influenced by preload, contractility, and afterload.
Preload: the volume of blood that fills a newborn's heart ventricles at the end of the heart's resting phase (diastole), just before the heart muscle contracts
Contractility: the strength and vigor of a newborn's heart muscle contraction
Afterload: the pressure or resistance that a newborn's heart must overcome to pump blood out of the ventricles and into the rest of the body
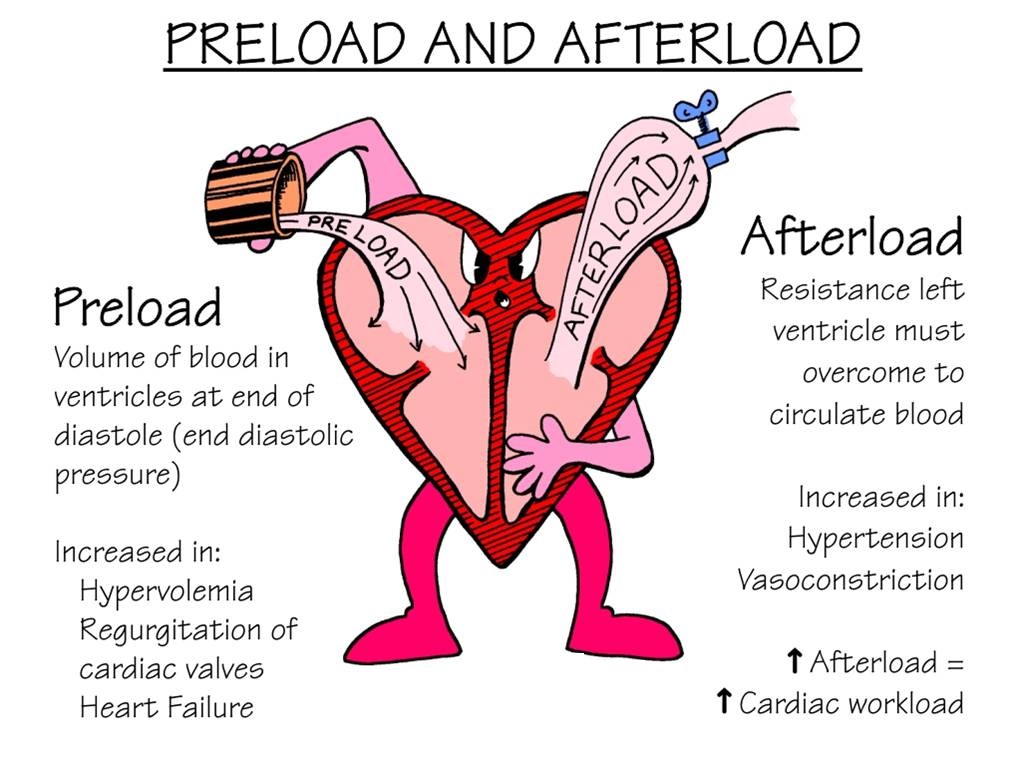
Image credit: FACMedicine
It doesn't end there....
Of course we care about cardiac output, but why? The heart pumps blood in order for it to carry oxygen to the tissues. Oxygen delivery (DO₂) depends on cardiac output and arterial oxygen content (CaO₂). C\
.Oxygen Delivery (DO₂) = Cardiac Output × Arterial Oxygen Content (CaO₂)
Another important concept, is oxygen consumption. How much oxygen is the tissue using to maintain normal metabolism?
Oxygen Consumption (VO₂) stays stable until oxygen delivery drops below a critical threshold.
When delivery can’t keep up, tissues increase oxygen extraction. Once that maxes out, metabolism shifts from aerobic (efficient ATP production) to anaerobic, producing lactic acidosis.
⚠️ What Happens During Shock?
Shock develops when tissue oxygen demand exceeds supply. Early on, the neonate compensates with tachycardia, vasoconstriction, and preferential blood flow to vital organs (heart, brain, adrenal glands). But as compensation fails, perfusion drops, anaerobic metabolism takes over, and lactate rises.
RNC tips:
Neonates can only really increase their CO by increasing their HR
increasing lactate is a hallmark sign of inadequate tissue oxygenation
In neonates, this process is even more complex:
Transitional circulation (open ductus arteriosus, immature myocardium) alters normal physiology
Prematurity further limits the heart’s ability to increase stroke volume, making cardiac output heavily rate-dependent
Organ immaturity means subtle changes in preload, afterload, or contractility can quickly tip the balance and overwhelm the heart.
👩🏻⚕️Clinical Assessment Beyond Blood Pressure
Effective shock management requires comprehensive hemodynamic assessment:
Tissue perfusion markers including lactate levels and capillary refill
Organ-specific perfusion assessment (NIRS, urine output)
Volume status evaluation
Cardiac output evaluation through functional echocardiography
Recent evidence suggests that isolated hypotension without signs of poor perfusion may not require immediate intervention, particularly when cardiac output compensates for decreased vascular resistance.
📚Evidence-Based Treatment Approaches
Current research highlights several important considerations:
Volume Expansion: Multiple studies question the routine use of fluid boluses in preterm infants. Evidence suggests limited benefit and potential harm, including increased risk of intraventricular hemorrhage.
Vasopressor Selection: The choice between dopamine, epinephrine, and other agents should be guided by the underlying pathophysiology.
For example:
Dopamine may be preferred when both inotropic and vasopressor effects are needed
Epinephrine might be superior for pure myocardial dysfunction
Vasopressin could be considered for vasodilatory shock
Corticosteroids: Low-dose hydrocortisone has shown efficacy in vasopressor-resistant hypotension, particularly in extremely preterm infants with relative adrenal insufficiency.
👶The Importance of Individualized Care
Perhaps the most critical takeaway from current research is the need for individualized assessment. Population-based blood pressure norms serve as guidelines, but each patient requires comprehensive evaluation of their hemodynamic status. The goal is not simply to normalize blood pressure, but to ensure adequate oxygen delivery to vital organs.
As NICU nurses, understanding these physiological principles helps us advocate for appropriate monitoring, recognize when intervention is truly needed, and support evidence-based treatment decisions. The complexity of neonatal shock demands sophisticated assessment skills and collaborative care approaches.
Ready to deepen your understanding of neonatal shock and vasoactive medications?
I'm so excited for my upcoming mini-course: "Neonatal Shock & Vasoactive Drugs: Advanced Concepts for NICU Nurses." This comprehensive course will cover:
Detailed shock pathophysiology
Evidence-based assessment techniques
Pharmacology of vasoactive medications
Case-based learning scenarios
Latest research applications
The full course won't be available until the end of October, but you can pre-order the course today!
P.S. If you pre-order, you will receive some bonus materials to help you at the bedside before the full course is out!
I'm Ready! Click Here to Pre-Order
Missed my other newsletters? Click here to read them!
References:
Lakshminrusimha, S., Seri, I., & Noori, S. (2024). Pathophysiology and etiology of neonatal shock. In R. A. Polin & S. H. Abman (Eds.), Fetal and neonatal physiology (6th ed.). Philadelphia, PA: Elsevier .
Noori, S., Seri, I., & Kluckow, M. (2024). Cardiovascular compromise in the newborn infant. In R. A. Polin & S. H. Abman (Eds.), Fetal and neonatal physiology (6th ed.). Philadelphia, PA: Elsevier .
Noori, S., Friedlich, P. S., & Seri, I. (2022). Pathophysiology of shock in the fetus and neonate. In R. A. Polin & S. H. Abman (Eds.), Fetal and neonatal physiology (5th ed.). Philadelphia, PA: Elsevier .
Kumar, V. K., Pandita, A., Reddy, V. V., & Thakur, D. (2025). Neonatal shock: Current dilemmas and future research. Children, 12(2), 128. https://doi.org/10.3390/children12020128


December 2023 Certification Review Webinar
NICU Certification Review


Ready to kickstart your journey to becoming a certified NICU nurse?
Look no further!
Grab my FREE E-Book packed with essential study and test-taking strategies for the RNC-NIC.
In the E-Book I give you the resources you need including the link to access the candidate guide, several types of books to study from, some of my favorite strategies, an outline of the content you should review, and a blank calendar for you to make your study plan!
Frequently Asked Questions About the RNC-NIC exam

What is the RNC-NIC?
The RNC-NIC is a competency-based exam that tests the specialty knowledge of nurses in the United States & Canada who care for critically ill newborns and their families.
The RNC-NICU is a nationally recognized certification that recognizes the registered nurse for their specialty knowledge and skill.

Who can take the RNC-NIC exam?
Nurses can take this exam after a minimum of two years experience in the NICU caring for critically ill newborns and their families.

Which books should I use?
I'm glad you asked! There are many excellent books to help you prepare for the RNC-NIC, I gathered ande describe each of them for you in my FREE e-book.
Is there a course to help me study?
Yes! Many hospitals host their own certification course and there are a few online courses. See my RNC-NIC test taking tips E Book for more information
What happens if I don't pass the exam?
If you don't pass the exam on your first try you can try again after 90 days. You will have to reapply after 90 days and pay a retest fee. There is no limit to the number of times you can take the exam (however a candidate can only sit for the exam twice per year).

Can I make more money if I take the RNC-NIC exam and get certified?
Yes! Many hospitals provide a raise or a bonus for nurses with specialty certifications. Hospitals also typically hire at a higher base salary when nurses have a certification.

Find me @amandasnicued on these channels or Email me
hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]